Despite seeming similar, the terms ventilation and oxygenation relate to two separate (albeit interdependent) physiological processes. Understanding the difference between the two is critical in being able to effectively treat patients and make appropriate clinical decisions (Galvagno 2012).
When confronted with a patient who is having respiratory difficulties, it is important to know whether they need help ventilating (getting air in and out of their lungs), or if they need oxygen due to hypoxaemia (impaired gas exchange).
Early detection of respiratory decline reduces the incidence of medical emergencies, the need for mechanical ventilation and the need for intensive care unit admission. Therefore, having adequate knowledge about respiratory anatomy and physiology means you will be able to respond to patients correctly and hopefully prevent deterioration (Vincent et al. 2018).
What is the Difference Between Ventilation and Oxygenation?
Ventilation
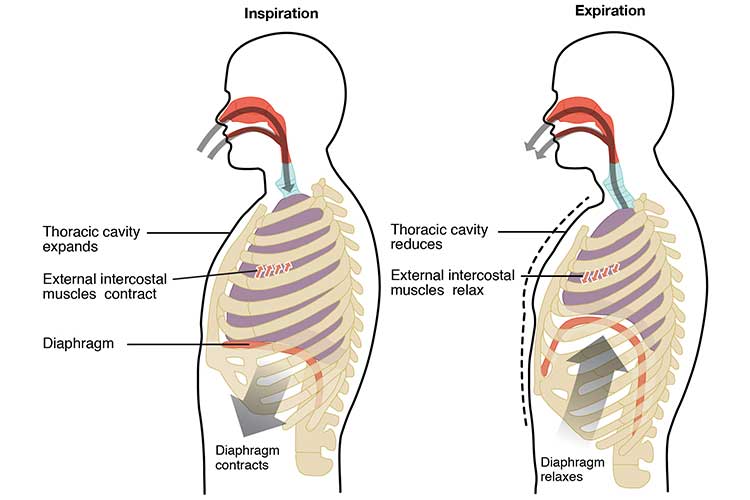
Ventilation can be considered the act of normal, spontaneous breathing. It refers to the two processes of inspiration and exhalation, i.e. the movement of air in and out of the lungs. (Pandirajan 2022).
These processes form a delivery system that provides the alveoli with oxygen-rich air (Reminga & King 2016).
Inspiration is initiated by the contraction of the inspiratory muscles (diaphragm and external intercostal muscles), which increases the volume of the thoracic cavity and subsequently the lungs. This creates a negative pressure that allows the air to be easily drawn into the lungs (Pandirajan 2022).
Expiration is the opposite process, wherein the inspiratory muscles relax and cause the volume of the thoracic cavity and lungs to decrease. This creates a positive pressure that forces the air to move out of the lungs (Pandirajan 2022).
Ventilation can be measured by assessing clinical signs (chest rise, compliance and respiratory rate) (Galvagno 2012).
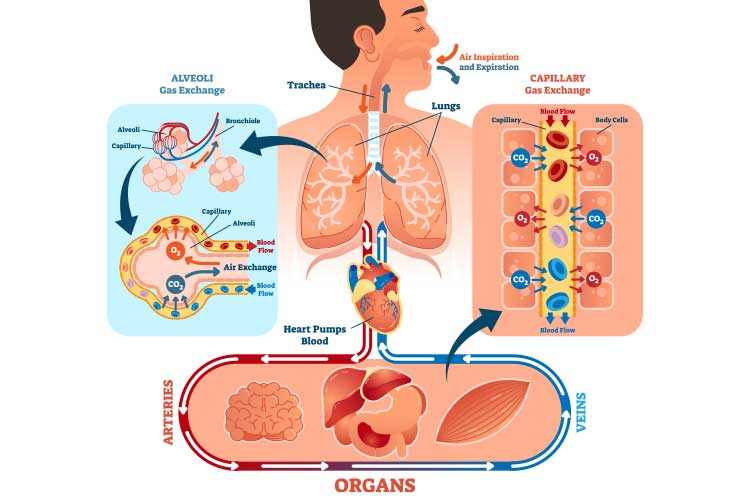
Oxygenation is the delivery of oxygen to the tissues to maintain cellular activity (Reminga & King 2016).
It is part of the gas exchange process, wherein oxygenation occurs simultaneously with the elimination of carbon dioxide from the bloodstream to the lungs (Dezube 2023; Kaynar 2020).
These gases (oxygen and carbon dioxide) are transported through passive diffusion across the membrane, meaning the gas exchange process requires no energy expenditure from the individual (Wagner 2015).
Oxygenation can not be measured by assessing clinical signs alone; it generally requires a pulse oximeter (Galvagno 2012).
Gas exchange is a process wherein oxygenation occurs simultaneously with the elimination of carbon dioxide from the bloodstream to the lungs.
Respiratory Failure
Understanding the difference between ventilation and oxygenation is crucial when managing a patient experiencing respiratory failure - which is caused by an inability to maintain blood oxygen levels (hypoxia), an excessive amount of carbon dioxide levels in the blood (hypercapnia), or both at once (Knott 2020; MedlinePlus 2020).
There are four types of respiratory failure:
Type I (hypoxaemia), an oxygenation issue causing low oxygen and normal to low levels of carbon dioxide
Type II (hypercapnia), a ventilation issue causing low oxygen and high levels of carbon dioxide
Type III (perioperative)
Type IV (shock).
(Shebl et al. 2023; Cleveland Clinic 2023)
In order to appropriately respond to a patient, you need to determine the kind of difficulty they are facing.
Type I, also known as hypoxaemic respiratory failure, occurs when an individual is unable to oxygenate adequately. It is clinically defined by an arterial oxygen tension (PaO2) of less than 60 mmHg (on room air). Carbon dioxide levels are normal or low. It is the most common type of respiratory failure (Kaynar 2020).
Type I is generally associated with acute lung diseases that cause fluid or sputum to occupy the alveoli (oxygen cannot swim through fluid or infection) or collapse of alveolar units (Kaynar 2020).
Oxygen therapy is generally required to treat patients with hypoxaemia (Shebl et al. 2023).
Hypoxaemia is generally treated with oxygen therapy.
Type II Respiratory Failure (Hypercapnia)
Type II, also known as hypercapnic respiratory failure, occurs when there is excess carbon dioxide in the bloodstream. This is usually caused by hypoventilation, i.e. the patient is unable to ventilate adequately enough to draw in the amount of oxygen needed. This results in unbalanced gas exchange, causing carbon dioxide to accumulate (Patel et al. 2022; Jewell 2023; Malhotra 2012).
It is clinically defined by an arterial carbon dioxide pressure (PaCO2) of over 50 mmHg and may occur along with hypoxaemia (Shebl et al. 2023).
Ventilatory support (invasive or non-invasive, depending on the clinical situation) is generally required to treat patients with hypoxaemia (Shebl et al. 2023).
Type II respiratory failure is caused by conditions that impede ventilation, such as:
Hypercapnia is a medical emergency that can be fatal if untreated (Brody 2021).
Hypercapnia is generally treated with ventilatory support (invasive or non-invasive).
Conclusion
Patients experiencing respiratory failure will require appropriate intervention. It is crucial to differentiate whether it is a ventilation or oxygenation issue and treat the patient accordingly.
Care must be escalated to the medical team in the event of deterioration, as early intervention is vital to ensure the risk of mortality is decreased and invasive ventilation (if needed) is minimised.
Vincent, J et al. 2018, ‘Improving Detection of Patient Deterioration in the General Hospital Ward Environment’, Eur J Anaesthesiol., vol. 35 no. 5, viewed 1 May 2023, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5902137/
Wagner, PD 2015, ‘The Physiological Basis of Pulmonary Gas Exchange: Implications for Clinical Interpretation of Arterial Blood Gases’, European Respiratory Journal, vol. 45 no. 1, viewed 1 May 2023, https://erj.ersjournals.com/content/45/1/227
 New
New