Identifying Pain in Those Who Can’t Communicate It
CPDTime.
10m
Updated 12 Jun 2023
For patients who do not have the capacity to communicate, pain can be overlooked, causing significant but unnecessary discomfort and distress.
Defining Pain
Pain is complex, subjective and varying. The International Association for the Study of Pain (2022) defines pain as ‘An unpleasant sensory and emotional experience associated with, or resembling that associated with, actual or potential tissue damage’.
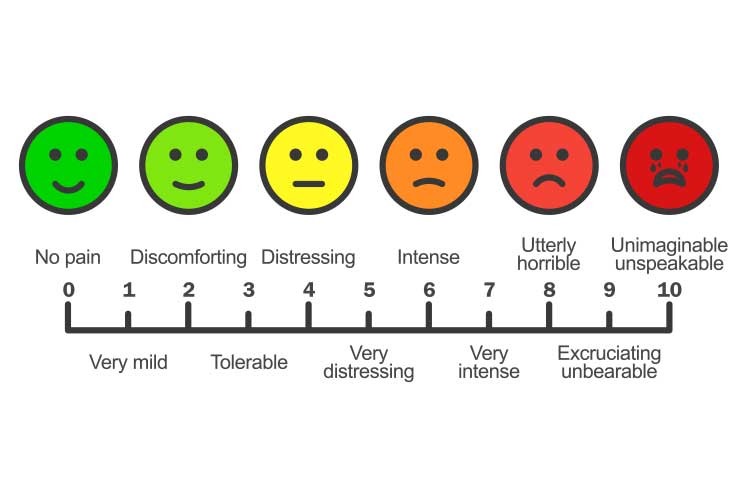
Pain can range from mild to severe, affecting a localised area or several parts of the body. It is a highly personal experience that varies in intensity depending on the individual, even if caused by the same stimulus (Shiel 2018).
In addition to causing physical discomfort, pain can also have implications on an individual’s emotional or mental wellbeing as well as their daily life (Healthdirect 2021).
Pain can be acute or chronic:
Acute pain is usually temporary and sudden, with a clearly defined trigger. It eventually resolves once the underlying cause has been addressed.
Chronic pain is persistent, often lasting for weeks, months or years. It may be triggered by an underlying condition, be a condition in its own right, or have no clear cause.
(Shiel 2018; Healthdirect 2021)
Pain Statistics
Pain is prevalent, especially among older adults and people living with medical conditions.
One in five Australians over 45 are living with chronic pain.
One in three adults over 65 are living with chronic pain.
Up to 80% of aged care residents are living with chronic pain.
(AIHW 2020; Painaustralia 2021)
People living with the following conditions have reported experiencing chronic pain:
Alzheimer’s disease and other types of dementia
Effects of stroke
Chronic lung disease
Cancers
Asthma heart disease
Diabetes
Osteoporosis
Mental illness
Hypertension
Arthritis
Other long-term conditions or injuries.
(AIHW 2020)
Communicating Pain
Patient self-reports are the most reliable gauge of pain.
The highly subjective nature of pain means that the best person to measure and describe the pain is the individual experiencing it. Patient self-reports are the most reliable gauge (Shiel 2018).
However, some patients may not have the capacity to self-report their pain. The process of discussing and assessing pain is a complicated social transaction between patient and healthcare professional, and if the patient is unable to communicate their pain, it becomes difficult to appropriately respond to and treat their discomfort (Boekel et al. 2017).
A study found that 1 in 10 patients self-report a low level of pain even if the pain is considered unacceptable. This poses serious questions and concerns about those who cannot communicate their pain at all (Boekel et al. 2017).
In addition to being a physically uncomfortable experience, untreated pain may also:
Cause unnecessary suffering
Worsen cognitive impairments
Cause the patient to become agitated
Impair the patient’s quality of life
Delay recovery
Interfere with daily life
Cause psychological distress
Cause breathing difficulties leading to respiratory deterioration
Cause immobilisation
Impair physical function
Increase the risk of falls.
(Booker & Haedtke 2016; McGuire et al. 2016; Gan 2017)
When a patient is unable to verbally express their discomfort, you should use assessment tools and observe for any pain behaviours. This is imperative to ensure all patients are comfortable and nobody is unknowingly suffering (Booker & Haedtke 2016).
Who Might be Unable to Communicate Pain?
Post-anaesthetic patients
Patients with cognitive impairment (e.g. dementia)
Patients receiving palliative care
Patients receiving end-of-life care
Deaf or hard of hearing patients
Intubated patients
Sedated or unresponsive patients
Patients with aphagia
Neurologically compromised patients
Patients who have fears, beliefs and misconceptions about their pain
Patients who have specific cultural needs
Patients who have difficulty with literacy and numeracy skills.
(Booker & Haedtke 2016; McGuire et al. 2016; Marie Curie 2022; Health.vic 2021)
There are several reasons why a patient may be unable to communicate their pain.
Non-Verbal Pain Assessment Tools
There many tools that may be used to assess non-verbal patients. The following are some widely-used examples - please note that this is not a comprehensive list of every tool available.
Note: Always refer to your facility’s policies and procedures when selecting and using pain assessment tools.
Non-Verbal Clinical Signs and Symptoms of Pain
The following behaviours may suggest the presence of pain in adults who are unable to communicate:
Facial expressions
Rapid blinking, fear, brow lowering, clenched teeth, narrowing or closure of eyes, upper lip raising, nose wrinkling.
Verbalisations
Screaming, swearing, crying, moaning, sighing, making fewer sounds than is typical.
Body movements
Gaiting, limping, rubbing a body area, muscle rigidity, decreased movement, guarding, pacing, rocking, fidgeting, repetitive movements, reluctance to move, decreased range of movement.
Interpersonal interactions
Resisting care, aggression, withdrawal, isolation.
Wandering, sleep disturbances, increased sleep, social disengagement, change of routine, staying in bed, low appetite.
Function
Decreased ability to function in daily life, falls.
Autonomic signs
Pallor, altered breathing, change in vital signs, sweating.
(Adapted from Booker & Haedtke 2016; Dementia Australia 2015)
Note: These signs may be unrelated to pain and caused by another condition. Some patients experiencing pain may display few or none of these signs (Dementia Australia 2015).
When a patient is unable to verbally express their discomfort, you should observe for any pain behaviours.
Challenges Faced by Healthcare Professionals
A study identified the following challenges experienced by nurses that may inhibit the assessment of pain in non-verbal patients:
Pain assessment of non-verbal patients not being routine
Lack of relevant policies and procedures
Inadequate discussions about pain between nurses and physicians
Lack of assessment tools in the nursing flowchart
Inadequate nurse-to-patient ratios
Limited or no experience in using non-verbal assessment scales
The belief that sedated patients do not need additional pain relief
Lack of understanding regarding pain in unconscious patients
The belief that non-verbal assessment tools are ineffective
Unfamiliarity with non-verbal pain scales
Lack of training in non-verbal pain scales.
(Deldar et al. 2018)
Identifying and remedying these barriers to effective pain assessment will help improve the quality of care delivered to non-verbal patients (Deldar et al. 2018).
Conclusion
Sourcing and using appropriate assessment tools for patients who are unable to communicate their pain is crucial. Poorly-managed pain can lead to other health complications and unnecessary discomfort and distress.
Thorough assessments should be performed to identify and manage pain experienced by non-verbal patients - being unable to verbalise their discomfort means they are relying on healthcare professionals to ensure they are comfortable and not quietly suffering.
McGuire, DB, Kaiser, KS, Haisfield-Wolfe, ME & Iyamu, F 2016, ‘Pain Assessment in Non-Communicative Adult Palliative Care Patients’, Nurs Clin North Am., viewed 6 June 2023, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4978178/
 New
New