This article is a compilation of guides on assessing lung, heart and bowel sounds.
Lung Sound Assessment
From the general practice to the ICU, listening to lung sounds can tell you a great deal about a patient and their relative health. However, knowing the difference between rales, a crackle, and a wheeze is sometimes still a confusing proposition for many health professionals, especially new grads.
Part of the reason for that is that some of the language is interchangeable (for instance, crackles and rales).
Knowing how to correctly identify adventitious breath sounds can tell you, and the other members of the care team, a lot about a patient’s condition.
Rhonchi and Wheezes
1. Sonorous Wheezes (Rhonchi)
What was once called ‘rhonchi’ are now mostly referred to as sonorous wheezes (though the terms are still used interchangeably). Sonorous wheezes are named thusly because they have a snoring, gurgling quality to them, or are similar to a low-pitched moan, more prominent on exhalation.
Sonorous wheezes are caused by blockages to the main airways by mucous secretions, lesions or foreign bodies. Pneumonia, chronic bronchitis and cystic fibrosis are patient populations that commonly present with rhonchi.
Coughing can sometimes temporarily clear this breath sound and alter its quality.
2. Sibilant Wheezes (Wheezes)
Formerly referred to as simply ‘wheezes’, sibilant wheezes are very closely related to the sonorous wheeze. Sibilant wheezes differ from sonorous wheezes as they are a higher-pitched, shrill, continuous whistling sound that occurs when the airway becomes obstructed and narrowed. These are the typical wheezes heard when listening to an asthmatic patient.
Crackles, also known as alveolar rales, are the sounds heard in a lung field that has fluid in the small airways. The sound crackles create are fine, short, high-pitched, intermittently crackling sounds.
The cause of crackles can be from air passing through fluid, pus or mucous. They are commonly heard in the bases of the lung lobes during inspiration.
Crackles can be further categorised as coarse or fine:
1. Fine Crackles
The sound quality of fine crackles is similar to the sound of hair rubbed between your fingers near the ear and may be heard in congestive heart failure and pulmonary fibrosis.
2. Coarse Crackles
Coarse crackles are lower-pitched and moist-sounding, like pouring water out of a bottle or ripping open velcro. This lung sound is often a sign of adult respiratory distress syndrome (ARDS), early congestive heart failure, asthma or pulmonary oedema.
Stridor
Stridor is a continuous, high-pitched crowing sound heard predominantly on inspiration, over the upper airway. Stridor may be a sign of a life-threatening condition and should be treated as an emergency situation.
Stridor usually indicates the partial obstruction of the larger airways, such as the trachea or a main bronchus, and requires immediate attention. It is also the most common type of breath sound heard in children with croup, though it is important to differentiate between croup and a foreign body airway obstruction.
It’s typically loudest over the anterior neck, as air moves turbulently over a partially-obstructed upper airway.
Pleural Friction Rub
A pleural friction rub is caused by the inflammation of the visceral and parietal pleurae. These membranes are usually coated in a protective fluid, but when inflamed, they stick together and make a sound like a harsh grating or creaking. A pleural friction rub often causes a great deal of pain, and the patient will splint their chest and resist breathing deeply to compensate.
A pericardial rub and a pleural rub will often sound similar, and the best way to distinguish between the two is to make the patient hold their breath. If you still hear the rubbing sound, then the patient has a pericardial rub and requires a different treatment.
Potential causes include pleural effusion and pneumothorax. A pleural friction rub is best heard in the lower anterior lungs and lateral chest during both inspiration and expiration.
Chest Sound Assessment
Depending on your specialty, your cardiac assessment probably consists of listening to an apical pulse over the mitral valve and sagely nodding your head.
It’s been years since you’ve thought about heart sounds, and in all honesty, they were kind of confusing to begin with. There was all that ‘lub’ and ‘dub’ and diastole and systole - enough to make a nursing student’s head spin round.
However, if you take the time to listen to them, heart sounds can actually tell you a great deal about a patient.
Instead of settling for good old ‘lub-dub’, put that stethoscope to greater use and reacquaint yourself with the sound of the heart.
Okay, let’s make this simple. We are going to listen to the heart over the valves and nothing more. No Erb’s point or anything esoteric. It just doesn’t matter in your everyday assessment. Now, if you hear a murmur over the valve… we are getting somewhere.
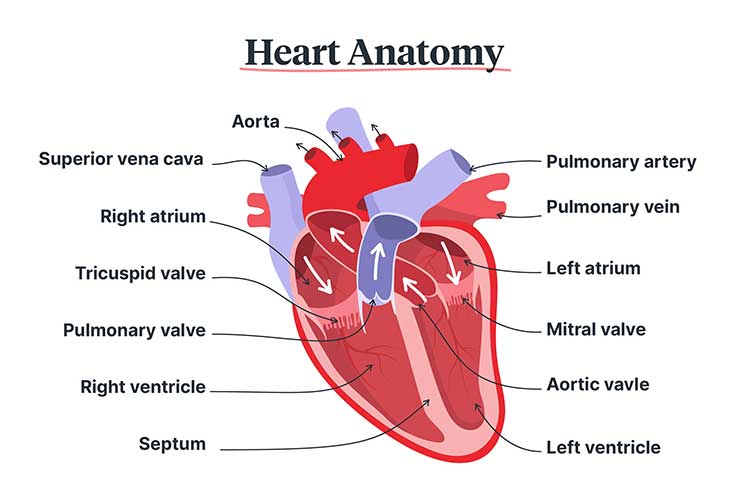
You know there are four valves in your heart: aortic, pulmonic, tricuspid and mitral. It helps to think of them in this order. They make a sort of elongated ‘z’ on the chest, with the aortic valve starting at the top right and two intercostal spaces down at the sternal border.
The pulmonic valve is easy enough to find. It’s right across the sternum at the left sternal border.
To find the tricuspid valve area, stay on the left side and count down four intercostal spaces.
The mitral valve is relatively easy to find if you are used to taking an apical pulse. If not, go to the fifth intercostal space at the mid-clavicular line.
What Did I Just Hear?
Now that you know where to put your stethoscope, you have to make sense of what you are listening to. The first sound you hear in the cardiac cycle is the ‘lub’, and it is a sound full of meaning.
‘Lub’ means that the heart is in systole, or the ejection phase of the heart. It is the sound of the mitral and tricuspid valves closing as the body empties the ventricles into the lungs and body. It is also known as S1.
‘Dub’, or S2, is the beginning of diastole, or the relaxation phase of the heart. It is the sound of the aortic and pulmonic valves closing. During this time, the ventricles fill and the atria contract.
Occasionally, you may hear a ‘split’ S2 that sounds like ‘du-dub’. This is the aortic valve closing slightly before the pulmonic valve and is often a normal sound heard on inspiration. You can have a split S1 too when the mitral valve closes before the pulmonic valve, and it can sometimes indicate a bundle branch block. It is important to listen closely to hear when the sounds split.
What Does it Mean?
This is where most people’s eyes start to glaze over, but it is where you can learn something useful to your patient. You will need to listen to the heart with the bell of your stethoscope to hear the abnormal heart sounds.
To hear a ventricular gallop, or S3, you should listen over the mitral valve with the bell. It will sound like a weird plopping noise right after you hear the ‘dub’. The whole heartbeat will sound like the beats in the word ‘Kentucky’. This heart sound can indicate heart ischaemia or heart failure. The ventricles are stiffening and resisting the influx of blood in diastole. However, it is a normal sound in young adults under 30.
S4 is the heart sound for atrial gallop, and the heartbeat will sound like the beats in the word ‘Tennessee’. Listen over the mitral valve with the bell of the stethoscope. You will hear the plopping noise just before the ‘lub’ starts, which means it happens right before systole starts. This heart sound can tell you quite a bit. It is heard after heart attacks and can indicate aortic stenosis, ischaemia, heart failure and hypertension.
Heart Murmurs
Heart murmurs are the other heart sounds you will hear if you listen to enough hearts. They will often sound like the words ‘rush’ or ‘hush’ and can last throughout the heartbeat.
Some murmurs can be caused by stiff and narrowed valves that cannot tolerate the rapid flow of blood through them. Many people walk around with a murmur and experience no problems, but they may indicate something serious if they start suddenly, for example, heart failure, shock or a ruptured papillary muscle. Murmurs can also indicate ischaemia, infection, medicine toxicity and genetic disease in some cases.
Many cardiologists and cardiac nurses can pinpoint which valve the murmur comes from, when in the heart cycle it starts, and what grade the murmur rates. For those who are not so specialised, identifying that a murmur is present and calling it to the attention of the physician is likely all you need.
Bowel Sound Assessment
Most nurses carry out a cursory listen for bowel sounds, but you may not realise how variable and important these sounds can actually be.
As with most things learned at university, it is easy to forget the particulars once you are working on a nursing floor. Instead of really focusing on the sounds, you may simply write down what you think you hear.
This can be a problem because changes in bowel sounds may indicate problems with the patient long before other signs emerge. For instance, the absence of bowel sounds after surgery can indicate an ileus before the patient starts vomiting or complaining of abdominal pain.
For this reason, it is important to go over bowel sounds once more, pay closer attention to them, and not use them merely as a stepping stool to the next level of assessment. After reading this article, you may also like to review your knowledge of assessing constipation.
The Abdomen
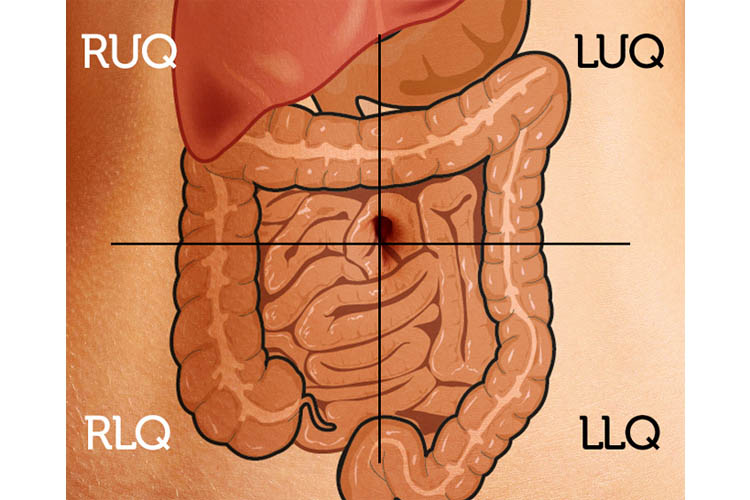
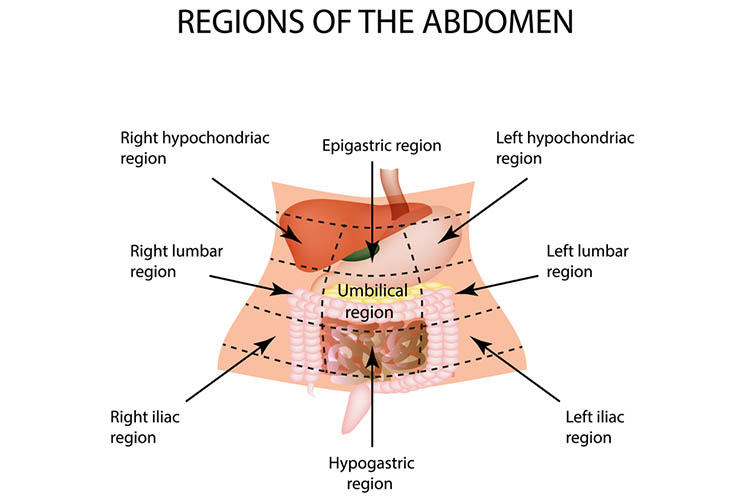
The abdomen can be divided into four quadrants. Although another system divides it into nine sections, the most common way to think of the abdomen is by drawing a line down the midline over the umbilicus and another across the abdomen, bisecting it at the same point. This will give you the standard right upper quadrant, right lower quadrant, left upper quadrant and left lower quadrant. You should know the structures within each area to help determine what the bowel sounds mean.
In the right upper quadrant, you will find the lower margin of the liver, the gallbladder, part of the large intestine and a few loops of the small intestine. The right lower quadrant contains the appendix, the connection between the large and small intestines and loops of bowel. The left upper quadrant contains the lower margin of the spleen, part of the pancreas and some of the stomach and duodenum. The left lower quadrant contains bowel loops and the descending colon. Knowing the structures under your stethoscope will help you determine the nature of the bowel sounds.
A diagram outlining the four quadrants of the abdomen. RUQ: right upper quadrant; RLQ: right lower quadrant; LUQ: left upper quadrant; LLQ: left lower quadrant.
What Bowel Sounds to Listen For
Although you can listen for vascular sounds over the abdomen, such as abdominal aortic bruits, most of the time, you are listening for the sounds of the bowels themselves. As peristalsis moves the chyme along the bowel tract, grumbling noises are heard, indicating that the bowels are active. You should listen over all four quadrants, not simply in one place. In fact, several areas per quadrant would be ideal, especially in patients who have gastrointestinal (GI) issues.
The first item to listen for is the presence of bowel sounds. To chart an assessment finding of no bowel sounds, you need to listen over the quadrant for at least five minutes. You should also do your auscultation before palpation and percussion to avoid influencing bowel sounds. In most cases, bowel sounds are present, but you need to categorise them. You should listen for the intensity of the sound - whether it is soft or strong. You should also listen for frequency. Hypoactive bowel sounds could indicate a problem, so if you are having trouble hearing them, this is significant.
Hyperactive bowel sounds, on the other hand, may indicate stomach upset, cramping and anything that is increasing peristalsis. The location and pitch of the sounds are important as well. Hypoactive bowel sounds in the right upper quadrant could indicate a bowel obstruction there. The pitch is important, too, as it can indicate the strength of the peristalsis and point to a problem.
What Findings Mean
Auscultating bowel sounds can allow you to pinpoint areas where an obstruction may have occurred. Finding no bowel sounds can mean an ileus or obstruction above that area of the intestine. Hypoactive bowel sounds are considered as one every three to five minutes, and this can indicate diarrhoea, anxiety or gastroenteritis. Hyperactive bowel sounds are often found before a blockage. It is quite common to find one quadrant with hyperactive bowel sounds and one with none or hypoactive ones. This is because the intestine is attempting to clear the blockage with increased peristalsis.
You may also hear high-pitched sounds and rushing noises. Again, this is a sign that the intestine is attempting to deal with a blockage. It is important to chart the location, quality, intensity and frequency of bowel sounds to document the GI system completely. Most nurses default to bowel sounds active in all four quadrants, but you need to be aware that this may not always be the case. A harried and hurried nurse may perform a quick assessment, but bowel sounds are a great indicator of the overall health of the patient. You need to listen for more than a few seconds and in several places to fully assess your client’s GI function.
Abdominal Assessment: Beyond Bowel Sounds
While listening for bowel sounds is important, that isn't the only way to assess this important part of the anatomy. You can inspect the area, palpate and percuss. However, you should probably listen to bowel sounds before manipulating the stomach, as this can cause changes in the way the sounds are heard.
The other three tools are important to fully assess the abdomen, though many nurses skip these parts and proceed directly to bowel sounds. By slowing down assessment and giving the abdomen the time and attention it needs, nurses can notice problems that may get past even the most experienced doctors.
Inspection
When assessing the abdomen, inspection is often overlooked. Merely looking at the abdomen can tell you a great deal about the patient and their relative health.
You should first look for symmetry to make sure there are no masses or protrusions that make one side of the abdomen bigger than the other.
This short video provides a four-minute overview of things to remember when performing a nursing assessment of bowel function in a palliative care setting.
You should also look for pulsation or movements under the skin. In very thin people, you will be able to see the movements of peristalsis, but you may also be able to see abnormal pulses of the descending aorta. This is important information.
You may also want to compare the abdomen to the rest of the body. If the stomach is large and the legs are thin, you may want to consider ascites. Similarly, if the legs are swollen and deformed, that swelling may continue on into the abdomen. You should also inspect the skin of the area, looking for dry patches or puckering of the skin.
In some patients with oedema, the abdomen may resemble the surface of an orange, and this can tip you off to a fluid imbalance issue.
Palpation
Palpation or feeling the abdomen is nearly as important as listening for bowel sounds. Many nurses gloss over this assessment, merely pressing on the stomach half-heartedly and moving on. However, you should take the time to really feel the abdomen. One of the first problems you may find is masses in the gut. You need to use your hands thoroughly to inspect the entire surface of the abdomen, looking for any masses, bulges, protrusions or abnormal spots in what should be soft tissue.
One of the problems with palpating the abdomen is eliciting a painful response from the patient. If they are complaining about abdominal pain and you deeply massage their abdomen, they are likely to squirm away from you. Still, it is important to feel the tissue for any abnormal signs.
One important part of palpation is guarding. You feel this when you attempt to palpate the abdomen but only feel resistance. This is because the patient is protecting their abdomen from pain, and it is a significant finding. Rebound tenderness is also important. You can find this by deeply palpating, removing your hands and watching for a pain reaction. Either of these should be reported to the physician.
Percussion
Percussion isn't used by any but the most advanced health professionals. In fact, physicians, nurse practitioners, and other nurses of advanced standing are probably the only ones who use this technique. There is a good reason for this: percussion of the abdomen can't tell you nearly as much as the other forms of assessment can, but it can shed some light on what's going on under that tissue. To percuss, you place two fingers over an area and knock on your fingertips with the fingertips of the other hand. This will allow the sound to travel through the tissue.
In the case of masses, percussion will sound different from normal bowel tissue. Most bowel sounds are rather hollow and empty, but a mass will have a thicker, duller sound. Blockages will sound different as well, and if you are unable to hear bowel sounds in a quadrant, it may be worth percussing over the area, searching for a blockage. Percussion is an inexact science, and it takes a fair amount of practice to get used to. You should try to percuss both the chest and abdomen of every patient you assess, but this isn't always possible. However, when you can, this practice will serve both you and the patient well in determining the source of their abdominal pain.
Topics
References
References
Estes, MEZ, Calleja, P, Theobald, K & Harvey, T 2013, Health Assessment and Physical Examination: Australian & New Zealand Edition, Cengage Learning Australia, South Melbourne, Victoria.
For Teams
Assign to your staff
Assign mandatory training and keep all your records in-one-place.
 New
New