Central Line-Associated Bloodstream Infections (CLABSI)
CPDTime.
7m
Updated 27 Apr 2023
What is a Central Line-Associated Bloodstream Infection?
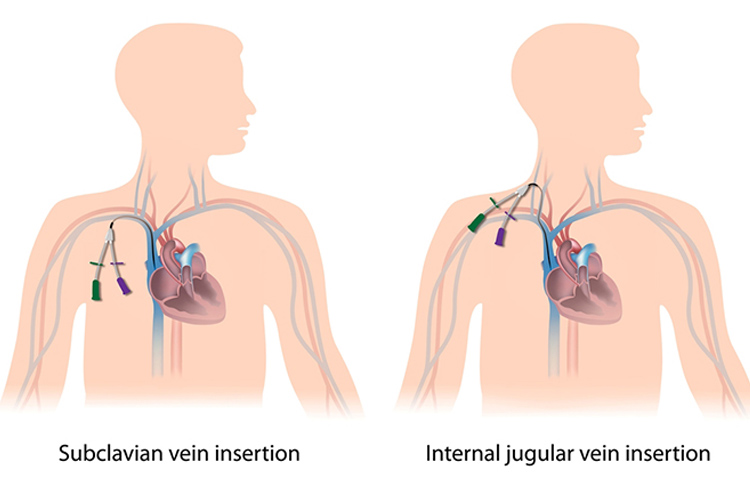
A central line, like the name implies, is a catheter that gains direct entry into the bloodstream with the tip of the line sitting either within the superior vena cava or inferior vena cava, or within one of the great vessels of the neck.
As a result of its central location, this type of catheter can occasionally allow pathogens to gain direct entry into the bloodstream. If this occurs, because of the location of the catheter, patients become unwell very quickly.
This is why prompt assessment, recognition and treatment of central line-associated bloodstream infections (CLABSI) are essential to help ensure favourable patient outcomes are achieved.
The Australian Commission on Safety and Quality in Health Care (ACSQHC) (2019) states that one of the following criteria needs to be met in order for a patient to be diagnosed with a CLABSI:
Criterion 1
✔
A patient of any age has a recognised bacterial or fungal pathogen cultured from one or more blood cultures.
✔
The organism cultured from blood is not related to an infection at another site.
OR
Criterion 2
✔
A patient of any age has at least one of the following signs or symptoms:
Fever (> 38°C)
Chills
Hypotension, or
A patient < 1 year of age has at least one of the following signs or symptoms:
Fever (> 38°C core)
Hypothermia (< 36°C core)
Apnoea
Bradycardia.
✔
The organism cultured from blood is not related to an infection at another site.
✔
The same (matching) potential contaminant organism is cultured from two or more sets of blood cultures drawn on separate occasions within 24 hours.
(ACSQHC 2019)
As you can imagine, the cost of CLABSI in both healthcare dollars and patient morbidity is high. Each CLABSI episode increases the length of the patient’s hospitalisation as well as substantially increasing the cost of their healthcare (Haddadin et al. 2022). Therefore, it’s important to be aware of the causes of CLABSI and how we can prevent them from occurring (ACSQHC 2019).
What Causes a Central Line-Associated Bloodstream Infection?
There are many different ways in which contamination of the central line can occur and cause infection. These include:
Contamination upon insertion
The patient’s skin flora
The healthcare professional accessing the central venous access device
Colonisation of the central venous access device (CVAD) hub
Contaminated infusion or components of the IV set
Haematogenous spread from other sites (e.g. through the bloodstream from another infection)
Non-intact dressing.
(Haddadin et al. 2022)
Patient-related risk factors for developing a CLABSI include:
Position of the central line (femoral and internal jugular catheters carry the highest risk)
Lengthy hospitalisation before venous catheterisation.
(Haddadin et al. 2022; Chopra et al. 2013; WHO 2016)
Other risk factors include:
Poor hand hygiene from healthcare workers
Non-adherence to aseptic non touch technique
Emergency catheter insertion
Non-compliance with central line maintenance, such as not using antiseptics or not completing dressing changes
Prolonged duration of the catheter.
(Haddadin et al. 2022; Chopra et al. 2013; WHO 2016)
Central Line-Associated Bloodstream Infection Symptoms
Central line related infections can be either localised or systemic.
Symptoms of localised infection may include:
Redness
Swelling
Discharge at the central line exit site.
(Haddadin et al. 2022)
If a localised infection is suspected, a swab can be taken from the central line exit site if exudate is present.
Symptoms of systemic infection may include:
Fever
Hypotension
Chills/rigors
Altered cognitive state.
(Haddadin et al. 2022; MedlinePlus 2022)
If a CLABSI is suspected, a full septic screen of the patient should occur. This will often involve the following investigations:
A set of blood cultures from each lumen of the CVAD
A set of blood cultures from peripheral blood
A swab of the central line exit site if there is exudate present
Vital signs
A full blood count
Electrolytes, urea and serum creatinine
Liver function
Midstream urine specimen
Chest x-ray
Sputum
Other wound swabs.
(Haddadin et al. 2022; ACSQHC 2019)
How are Central Line-Associated Bloodstream Infections Treated?
Treatment of a CLABSI needs to commence promptly. Specific management will depend on the causitive pathogen, patient factors and the patient’s overall clinical status. Blood cultures should be taken to identify the causative organism, and empiric treatment should be commenced while awaiting these results. Generally, antibiotics that cover both gram-positive and gram-negative bacteria will need to be administrred. Once blood culture results are available, more specific therapy can be commenced (Haddadin et al. 2020).
The CVAD may also be removed. If it is to be removed, then the catheter tip may be sent to pathology for cultures. Prior to removal, blood cultures may also be taken via the CVAD
(Haddadin et al. 2020).
Nursing Care and Central Line-Associated Bloodstream Infection Prevention
One of the most important factors of management of a central line is the nursing management of the device and the patient. This not only includes assessing the patient for risk factors for potentially developing an infection, but also means ensuring preventative measures are in place and management of the central line occurs using aseptic non touch technique.
The use of maintenance checklists as well as insertion bundles can also be used to standardise central line care and have been found to reduce the incidence of CLABSI from occurring (ANZICS 2019).
The nurse must manage the central line according to their local hospital policy and procedures, however, this management may include the following:
Hand hygiene
Disinfecting hubs, needle connectors and injection ports prior to CVAD use and as per protocol
Removing nonessential CVADs
Chlorhexidine cleansing as per protocol
Monitoring the CVAD dressing using chlorhexidine products and topical antibiotics
Antibiotic/anti-infective ‘locks’ in high-risk patients
Systemic antibiotic prophylaxis
Replacing administration sets other than those used for lipids or blood products every 96 hours.
(CDC 2015; Chopra et al. 2013; Haddadin et al. 2022)
Healthcare professionals should also educate patients in the management of their central line and how they can help protect themselves against a possible CLABSI. Encourage patients to:
Speak up about any concerns
Ask if the central line is absolutely necessary and how long it may be in place
Pay attention to the dressing around it (e.g. if it is wet or dirty)
Tell a healthcare worker if the catheter site is sore or red
Avoid touching the tubing as much as possible
Avoid letting visitors touch the tubing.
(CDC 2011)
The healthcare professional must also monitor for any signs or symptoms of a CLABSI, as well as other complications such as air embolism, catheter damage, catheter migration and occlusion.
In the management of central lines and prevention of CLABSI, the role of the healthcare professional is essential.
Centers for Disease Control and Prevention 2011, Central Line-associated Bloodstream Infections: Resources for Patients and Healthcare Providers, U.S. Department of Health & Human Services, viewed 19 April 2023, https://www.cdc.gov/hai/bsi/clabsi-resources.html
Chopra, V, Krein, SL, Olmsted, RN, Safdar, N & Saint, S 2013, ‘Chapter 10: Prevention of Central Line-Associated Bloodstream Infections: Brief Update Review’, Making Health Care Safer II: An Updated Critical Analysis of the Evidence for Patient Safety Practices, viewed 19 April 2023, https://www.ncbi.nlm.nih.gov/books/NBK133364/
Haddadin, Y, Annamaraju, P & Regunath, H 2022, ‘Central Line Associated Blood Stream Infections (CLABSI)’, StatPearls, viewed 19 April 2023, https://www.ncbi.nlm.nih.gov/books/NBK430891/
World Health Organisation 2016, ‘Core Components: Guideline Recommendation’, Guidelines on Core Components of Infection Prevention and Control Programmes at the National and Acute Health Care Facility Level, viewed 19 April 2023, https://www.ncbi.nlm.nih.gov/books/NBK401782/
 New
New