 New
New 12 Lead ECG Placement
CPDTime.
4m
Published: 10 June 2021


Published: 10 June 2021
An electrocardiogram, or ECG, is a reading assessing the magnitude and direction of the electrical currents of the heart, and measuring the depolarisation and repolarisation of the cardiac muscle cells (Medani et al 2018).
It is important an ECG is recorded accurately.
ECG electrode placement is standardised, allowing for the recording of an accurate trace - but also ensuring comparability between records taken at different times.
Poor electrode placement can result in mistaken interpretation, which may then lead to possible misdiagnosis, patient mismanagement or inappropriate procedures (Khunti 2013). Deviation of lead placement even by 20-25mm from the correct position can create clinically significant changes on the ECG, including changes to the ST-segment (McCann et al. 2007).
Patient factors such as respiration, position, smoking, recent dietary intake and obesity may also contribute to the accuracy of an ECG reading (McCann et al. 2007).
It is therefore important to not only ensure that the electrodes are placed in accordance with the standardised ‘rules’, but also, that the patient is prepared correctly for the procedure, both physically and psychologically.
As with all procedures, you must obtain informed consent from the patient by explaining the purpose of the procedure, describing the procedure itself and obtaining consent to proceed. Maintain good infection control practice by washing your hands prior to patient contact.
Skin preparation is important. If the patient’s skin is dirty, clean with soap and water, and then dry. If the skin is oily or the patient applied any creams or lotions, use an alcohol wipe to clean each electrode placement site.
Some ECG machines may also provide a ‘rough patch’ either separately or on the electrodes, which can be used to rub on the skin to increase electrode adherence. Care should be taken not to cause abrasions.
Patients with chest hair should have hair at the electrode placement sites removed with a hair clipper (Coviello 2016).
Where possible, place the patient in a supine or semi-recumbent position with their legs and arms uncrossed (QAS 2020). If this is not possible or is uncomfortable for the patient, it is acceptable to record the ECG in another position.
The patient must be completely relaxed. Ensure the environment is at a comfortably warm temperature (Jevon 2010). This will prevent muscular tension or movements from producing artefact on the ECG recording. Ensure the patient’s privacy and dignity: e.g. by closing the room door or drawing around the curtains.
The patient’s chest and all four limbs should be exposed in order to apply the ECG electrodes correctly.
There are different methods for identifying the correct landmarks for ECG electrode placement, the two most common being the ‘Angle of Louis’ Method and the ‘Clavicular’ Method (Crawford & Doherty 2010a).
ECG electrodes are colour-coded, and each is identified by a specific code that refers to its intended placement. There are two coding systems currently in use:
Both systems are described in the table below.
| Code (AHA) | Code (IEC) | Location | Colour (AHA) | Colour (IEC) |
|---|---|---|---|---|
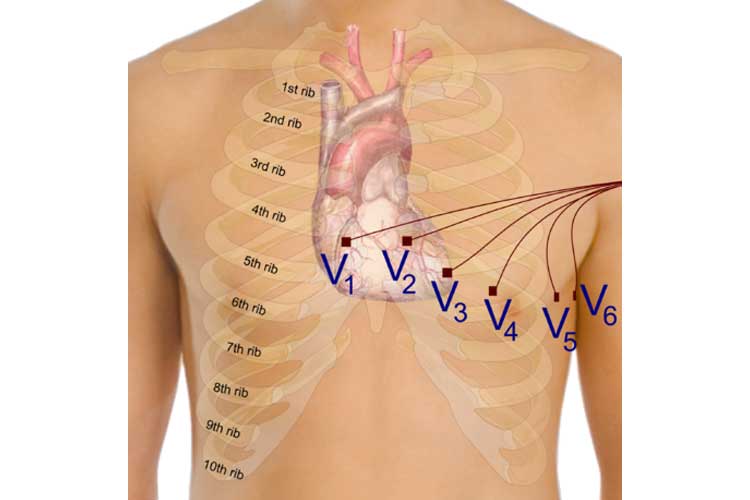
| V1 | C1 | Fourth intercostal space at the right sternal border | Brown/red | White/red |
| V2 | C2 | Fourth intercostal space at the left sternal border | Brown/yellow | White/yellow |
| V3 | C3 | Halfway between leads V2 and V4 | Brown/green | White/green |
| V4 | C4 | Fifth intercostal space in the midclavicular line | Brown/blue | White/brown |
| V5 | C5 | Left anterior axillary line on the same horizontal plane as V4 | Brown/orange | White/black |
| V6 | C6 | Left midaxillary line on the same horizontal plane as V4 and V5 | Brown/purple | White/purple |
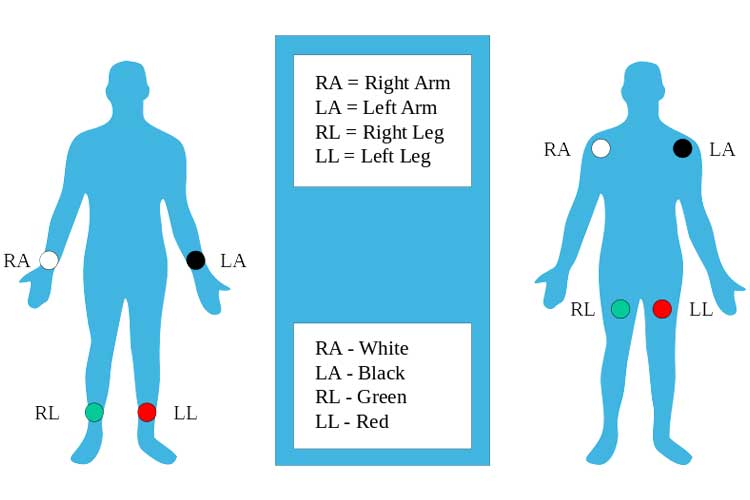
| RA | R | Right arm (inner wrist) | White | Red |
| LA | L | Left arm (inner wrist) | Black | Yellow |
| RL | N | Right leg (inner ankle) | Green | Black |
| LL | F | Left leg (inner ankle) | Red | Green |
(Adapted from Crawford and Doherty 2010a; Jevon 2010; Cables and Sensors 2016)
Note: The following guide uses the AHA system.
In order to find these correctly, the ‘Angle of Louis’ Method can be used:
(Coviello 2016)
Breast tissue can impact on the ECG amplitude due to the increased distance between the electrode and the heart when ECG electrodes are placed over the chest (Rautaharuju et al. 1998).
Therefore, in female patients, the V4, V5 and V6 leads are recommended to be placed underneath the left breast where the breast tissue meets the chest (QLD DoH 2012).
It is often customary in practice to write on the ECG if an electrode has been placed over breast tissue in order to aid the interpretation.
Where it becomes necessary, it is also customary practice to record any alterations in lead placement; for example, where lead placement is changed from the standardised location due to patient position, injury etc.
Ensure that the patient’s privacy and dignity are maintained. The chest should not be left exposed and can be covered back up with blankets, or the patient can re-dress as necessary.
The ECG electrodes should be removed if the patient is not likely to require further or serial ECGs, but otherwise can be left in place for up to 24 hours before needing to be replaced (Coviello 2016).
If you are not interpreting the ECG, follow local policy and use clinical judgement to arrange for interpretation. Local policies often also require the initials of the person taking the ECG to be recorded.


Ausmed Education is a Trusted Information Partner of Healthdirect Australia. Verify here.